May 2023
The Access to Healthcare Committee (A2HC) – formerly known as the Access to Healthcare Group – performed action research among relevant actors to better understand how the CityID could troubleshoot exclusion for undocumented people living in Amsterdam, as a case study in looking at wider exclusions.
In their practical, empirical investigation, A2HC (the committee consists of academics of the Vrije Universiteit – Athena Institute, researchers, activists, healthcare professionals and NGO actors) found that access to health was impeded due to complex implementation, discretionary practices and competing interests. When an individual does not have health insurance or a BSN (Burgerservicenummer), the healthcare provider only receives 80% maximum refund from the Centraal Administratie Kantoor (CAK). The healthcare provider struggles to find the right CAK budget type, and therefore may avoid providing care to undocumented patients. The patient may be asked to contribute to financial costs, including up to 500,- euros in case of emergency care; and finally, the undocumented individual may be unaware they are entitled to the Dutch healthcare system and rights, or faces language barriers in vocalising these rights.
Undocumented people in the Netherlands struggle to access basic and emergency healthcare, suffering from disproportionately high health issues, including unmet mental health and reproductive services needs (Schoevers et al., 2010; Vollebregt et al., 2022).
A study shows that health services remain significantly underutilised even if access is possible (Ataç, 2019; Hintjens et al., 2020). Meanwhile, an estimated 30 to 80 thousand undocumented persons reside in Amsterdam, composing a very heterogenous group; within this are even further marginalised groups, as a recent study of undocumented children in Amsterdam found 17% were not vaccinated, and 83% without a GP (Klok-Nentjes et a.l 2017).
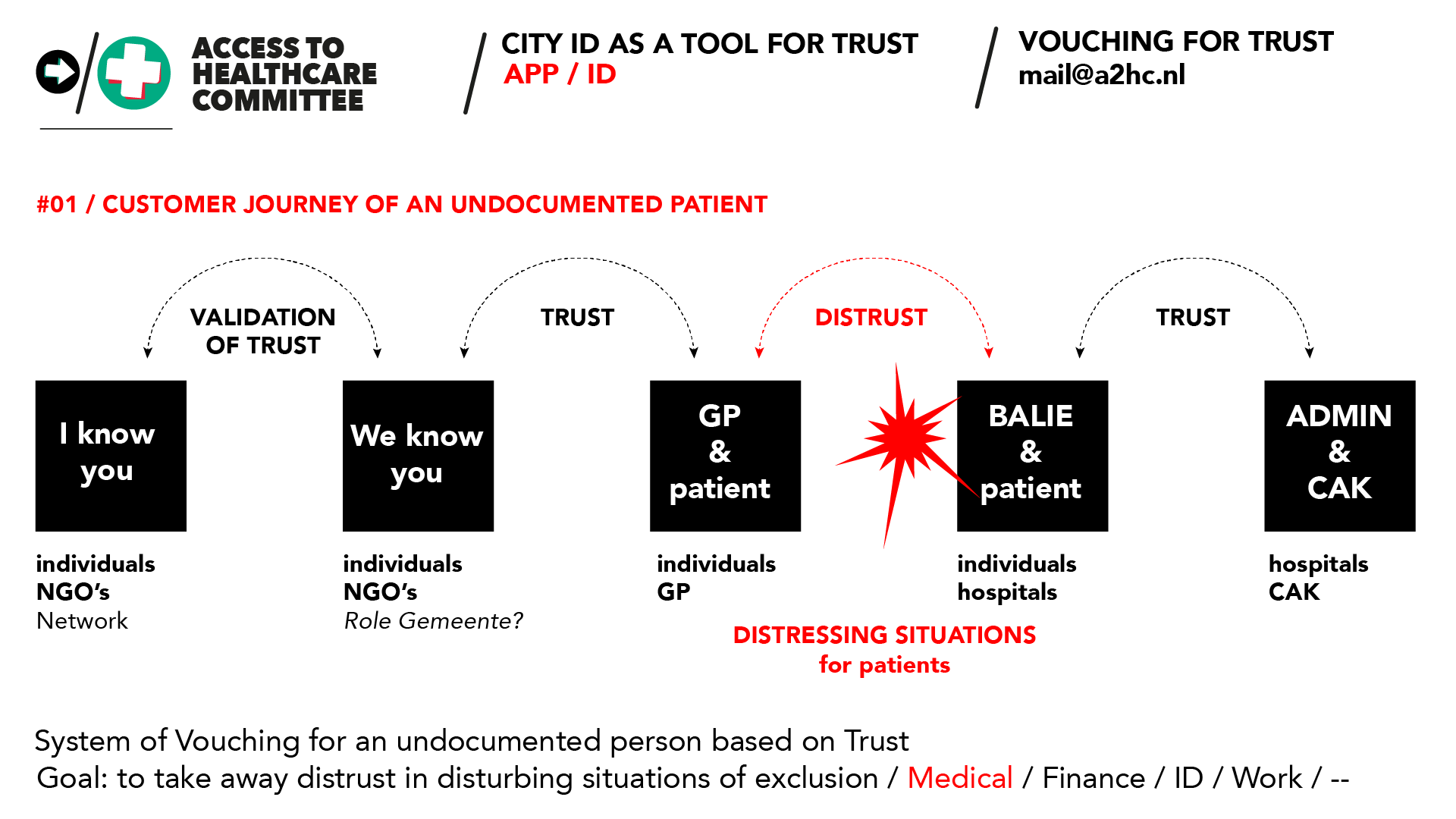
A2HC argues that to support access to health, on top of the paper process, a CityID offered via a digital wallet (app) with information on status may offer a solution in providing accessible healthcare for such a diverse and immensely marginalised group (and other excluded groups). By doing so, NGOs and a GP (General Practioner) could validate the undocumented person with regards to their identity and residence (rather than legal status) and the CAK budget type that applies. Meanwhile, the hospital could rely on the assessment of the Health Professionals and the NGO’s and provide care to the patients using the regular, standardised and optimised processes (including administrative), given its role of healthcare delivery and rather than supervising patient statuses (outside of medical status).
Access to Healthcare is fundamental right. How can a City ID facilitate this?
As such, the A2HC seeks to move forward with a design for proactive prevention of digital exclusion, as the City and wider European community move forward with digital identity. It primarily asks whether the municipality would be wiling to accept data from other organisations, subletting proofs, (i.e., in the illustrative case presented, NGOs or GPs) so that persons could use the ID to demonstrate and claim city residency. In moving forward in a multistakeholder, collaborative effort towards this goal, A2HC proposes a dialogue between city officials, health care providers, NGOs and advocacy organisations, researchers, the SSID and IRMA (YIVI) representatives, agreeing on a strategy.
We want to thank Henk Marsman for this report, stakeholder meeting May 30 2023 at the Vrije Universiteit Athena Institute.
Graphic by A2HC / 2023